The objective of the FAST exam: ”is to detect free intraperitoneal, intra-thoracic, and pericardial fluid in the setting of trauma.” When we perform the FAST exam the two questions we are trying to answer are:
- 1. Is there free fluid/blood in the abdomen?
- 2. Is there fluid/blood in the pericardium?
FAST is one of the easiest protocols to learn, it can be done very quickly (in a matter of minutes), and it can help detect potentially life-threatening conditions and therefore help decrease time to treatment.
Extended FAST (e-FAST) adds two additional questions:
- 3. Is there fluid/blood in the thorax?
- 4. Is there a pneumothorax present?
For the FAST exam there are three places we look for intraperitoneal fluid. The Right Upper Quadrant (RUQ), the Left Upper Quadrant (LUQ), and at the Suprapubic view. And to evaluate the presence of pericardial fluid, the place we look in the FAST exam is the subcostal cardiac view.
The FAST Exam, Probe & Orientation
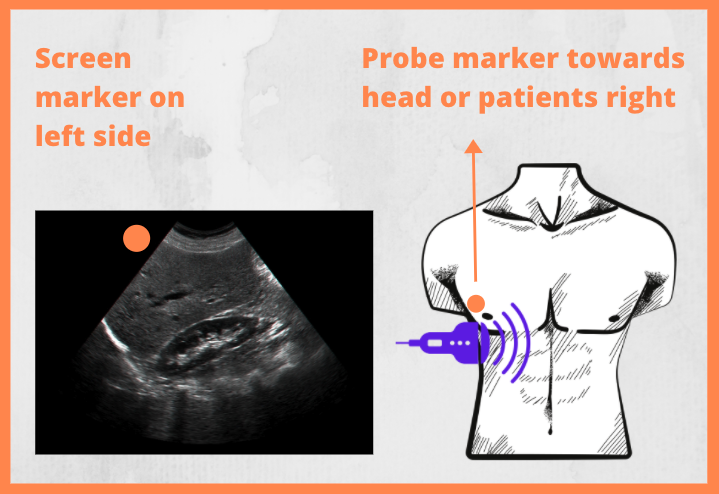
[Image credit: pocusbasics.org]
For most exams, including the FAST, the marker should always be turned towards the patients right or the patients head, with the screen image oriented towards the left from the viewers perspective (view image above). The probe most commonly used is either the curvilinear or phased-array probe, depending on the preference of the examiner. The curvilinear probe (also called the abdominal probe) provides a larger footprint and is easier to scan large areas with, while the phased-array (also called the heart probe) provides a smaller footprint and is therefore easier to scan in between ribs due to its size. Depending on the choice made, the same probe type can be used for the entire exam. Modern ultrasound machines also have pre-installed software with protocols that makes the image optimised for the FAST/abdomen evaluation and can be selected if/when using either probe.
3. FAST:RUQ
To obtain the image in the right upper quadrant, place the probe with the marker pointed towards the patients head, in the sagittal position, just below the ribs on the patients left side. The three areas you need to assess are:
- The space between the diaphragm and liver (probe gliding more towards the patients head)
- The space between the liver and the kidney, also called Morrison’s pouch (probe gliding more towards the middle)
- The space in the inferior/caudal part of the liver (probe gliding more towards the patients hip/feet)
When each area of focus is identified you’ll need to fan the probe in order to scan the entire space. Remember the image obtained on the screen is just a thin slice, by fanning you’ll visualize, slice by slice, the entire space of interest. If there is any free fluid, it’ll turn up as, most likely, anechoic (black) unless there’s a delayed trauma in which case it might portrait as more isoechoic (gray-scale) on the screen.
RUQ has the Highest Sensitivity for Diagnosing Free Fluid in the Intraperitoneal Space in the Setting of Trauma

[Image credit: Lobo et al. ‘Caudal Edge of the Liver in the Right Upper Quadrant (RUQ) View Is the Most Sensitive Area for Free Fluid on the FAST Exam.’ 2017.]
I sometimes get the question in what order FAST should be performed. My own recommendation is to begin with RUQ and the subcostal cardiac view when blunt trauma and no specific point of focus for injuries (such as with patients involved in motor vehicle accidents). Then LUQ and then finishing with the suprapubic view for FAST and then completing the exam with the two anteromedial E-FAST lung views for assessment of lung-sliding/PTX. The reasoning behind this is that RUQ has the highest sensitivity for free intraperitoneal fluid* and the subcostal cardiac view has a high yield for finding pericardial fluid. If there is signs of penetrating trauma to the chest I would suggest starting with the subcostal cardiac view as damage to the heart and pericardial fluid is (often) of higher clinical importance to assess than free fluid in the abdomen, and then to proceed with RUQ and LUQ both for free intraperitoneal fluid but also for signs of fluid in the pleura (i.e. a hemothorax) before finishing with E-FAST for PTX assessment and then the suprapubic view.
However, seeing as a complete E-FAST exam should take an experienced examiner approximately 2-3 minutes to finish and evaluate, the exact order of the examination is not always that important, especially not in a stable patient.
One retrospective cohort study from 2017 done in a trauma one center in California, including 1,008 scans, where 48 was positive (4,8%), found RUQ was the most positive view with 32/48 scans (66.7%) identifying free fluid in RUQ, and their sub-quadrant analysis found the caudal liver tip to be the most positive view in RUQ with 30 of those 32 positive RUQ views identifying free fluid in that space.* Note that in approximately one third of the positive FAST exams, free fluid was not found in RUQ, so a complete (E-)FAST should be done regardless (if the patient does not need immediate surgery) and since it only takes a couple minutes it can be done without delaying time to surgery significantly.
If RUQ however is positive the LUQ and suprapubic views become somewhat superfluous but can still help to some extent with your clinical assessment of the amount of free fluid in the intraperitoneal space. A complete FAST is also valuable, whether positive or not, if conservative treatment is decided upon and you do follow-up FAST exams if the patient is admitted for observation to see if free fluid has emerged/increased.
Double Line Sign (DLS)

[Image credit: Patwa et al. ‘Prevalence of the “double-line” sign when performing focused assessment with sonography in trauma (FAST) examinations.’ 2015.]*
As ultrasound machines get better and more sensitive for detailed imaging, there is a higher probability to misinterpreted benign signs for free intraperitoneal fluid. One of those signs is called the double line sign (DLS), and is a sign of perinephric fat. One study of 100 patients from 2015 found DLS to be present in 27% of the cases, there was no statistical significance among the different demographic groups or BMI. Note in the image from the study above: how perinephric fat (fig 1 asterix) is a wedge-shaped hypoechoic area in Morisson’s pouch that is bounded on both sides by echogenic lines, while free fluid (fig 2 upper arrow) has sharp edges, is often triangular in appearance and is only bound by an echogenic line on the renal border in Morrison’s pouch.*
4. FAST: LUQ
The left upper quadrant is obtained in a similar fashion but on the corresponding left side of the patient. However, due to anatomical differences, you’ll need to place the probe more posterior (towards the stretcher) and more cranially (towards the patient’s head). A rule of thumb is: ”knuckles to the stretcher”, meaning if you’re standing to the patient’s right and reaching over him, your knuckles might need to be posterior enough that they’re touching the bed.
In the LUQ there’s only two areas we need to assess:
- The space between the diaphragm and the spleen
- The space between the spleen and the kidney (the splenorenal recess)
In this view fluid is more commonly found between the spleen and the diaphragm, unlike the RUQ where fluid is most common found in Morrison’s pouch and/or the inferior liver edge.
7. Extended FAST
Extended fast includes the focused questions:
- 3. Is there a pneumothorax present?
- 4. Is there fluid/blood in the pleural cavity?
The extended part of FAST includes two apical lung projections looking for signs of a pneumothorax, and also looking for fluid in the pleural cavity by moving the probe towards the patients head in the RUQ and LUQ views. This helps us in the diagnostics of pneumothorax, hemothorax, and pneumohemothorax.
8. E-FAST:
Pneumothorax and the absence of lung-sliding

The orange arrow is pointing towards the pleural line, which is found below the ribs.In the image above lung-sliding is present.
[Image credit: Abhilash Koratala & NephroPOCUS.com]
For the additional two E-FAST views, place the probe approx on the middle of the patient’s pectoris, on either side of the sternum, above the mammillary line, at a 90 degree angle against the thorax, with the marker pointing upwards/cranially. The image we want to obtain is a crisp line (pleural line) between and below the two black circles (ribs) that cast shadows downwards on the screen (see image above). You don’t need to fan the probe in this position, however you might need to adjust the position of the probe a little in any fanning-direction if the pleural line is not clearly visualised, as you need to be at an exact 90 degree angle to get the best picture. For our purposes the only part of interest in the E-FAST exam protocol is the pleural line. How to understand and interpret lung ultrasound will be covered more in depth in the next module.
The visceral and parietal pleura glide against each other in correspondence to the patient’s breathing. This is referred to as ”lung sliding”. If the pleural line is still with no gliding occurring you should suspect that a pneumothorax might be present. Remember the simple principle of gravity: air rises, fluid sinks. With the patient lying on their back on the bed, air should be located and detected anteromedially (the “highest” point on either side) relative to their thorax. For the E-FAST exam it’s enough to look on either side of the patient’s sternum between a couple intercostal spaces as any pneumothorax that is large enough to be of interest in the primary survey of ATLS should be detectable in this space.
You might need to decrease the on-screen depth substantially for this exam in order to get a better view of the pleural line. You do not need to switch from a curvilinear probe to a linear one, even though the latter gives you better resolution, the former probe is more than sufficient to detect the absence of lung sliding and comes with two added benefits:
- You don’t need to waste time changing probes
- You can cover a bigger area in one image, often including more than a single intercostal space
If you’re having any difficulties judging whether there is lung sliding present or not, always remember that you also have a contralateral side to compare with. The presence of lung-sliding rules-out an pneumothorax in the space observed, however it does not rule-in a pneumothorax when absent as there can be other causes for the absent/decreased lung-sliding in that space.
There are other signs and methods for helping you determine if a pneumothorax is present, such as using ”M-mode” and looking for a ”lung point”. But as the E-FAST is part of a primary survey in ATLS and focuses on speed and quick assessment we will not cover that here, they will, however, be explained in the next section: M4 Lung Ultrasound.
Video PTX (5min):
[Credit: Jacob Avila & 5minsono.com]
9. E-FAST:
Hemothorax and the presence of spine-sign

[Image Credit: NephroPOCUS, The ‘Spine sign’]
In the RUQ and LUQ, when visualizing and centering the diaphragm, you can, by directing/fanning the probe towards the patients spine, visualize the spine on screen. The spine, or more often than not the ribs coming from the spine, will be seen as a hyperechoic chain connecting to the diaphragm (see image above, contrasting spine sign in the right image to the absence of spine sign in the left image). The spine will not extend beyond the diaphragm since ultrasound waves can’t penetrate the air contained in the lungs. Instead what you might see is a curtain-sign as the breath will bring a shadow area over the diaphragm with each breath. Or what might be visualized will be a vague resemblance of the liver/spine on the opposite side of the diaphragm visualized on screen due to the mirroring effect.
However, when there is fluid present the spine will be visualized beyond the diaphragm, demarcated by a black/hypoechoic fill (see image), called the “spine sign”. That is pleural fluid, and in the trauma setting should be suspected to be blood until proven otherwise. The presence of “spine sign” can indicate a hemothorax just as the absence of “lung sliding” indicates a possible pneumothorax.
Video (i) E-FAST, HTX (8 min):
[Credit: Phillips Perera & SonoSite]
Video (ii) E-FAST, HTX spine-sign (3 min):
[Credit: Abhilash Koratala & NephroPOCUS.com]
10. Summary
In this module we reviewed the FAST exam that contains four windows: RUQ, LUQ, subcostal, and the suprapubic window (the only one which you need to evaluate in both short- and long-axis). We also looked at E-FAST that adds two additional windows for evaluating PTX and requires/incorporates a RUQ & LUQ assessment of pleural effusion. I would claim that it’s impossible to do a FAST exam without assessing pleura/hemothorax while evaluating RUQ & LUQ, so in practice the addition of the E-FAST exam is the antermedial lung views for assessing lung-sliding/PTX.
E-FAST/FAST is an exam that can be done in a matter of minutes and can provide valuable information in that short period of time. It should not delay other prioritized management in the ATLS-algorithm. This exam can also be valuable for clinical assessment over time and should be repeated when needed.
11. Pitfalls FAST
- FAST: is not sensitive for detecting retroperitoneal fluid
- FAST: is not sensitive for detecting fluids less than 500-800 cc (ml)
- FAST: can’t differentiate between fluids like blood vs ascites
- FAST: should not delay other prioritised surveys such as CT / operation (follow the ATLS algorithm)
- Remember the usefulness of repeated FAST exams when needed to follow and evaluate clinical changes
- Supra pubic view: usually more caudal than you’d think, remember: the only view that requires both a short- and long-axis, easier to get good images if the bladder is filled
- LUQ view: obtained by moving the probe more cephalic and posteriorly than the RUQ view, remember the adage: “knuckles to the stretcher”
- LUQ view difficulty: try switching to phased array probe to better navigate between ribs if you are not pressed on time and it doesn’t delay other prioritised surveys
- E-FAST & PTX: the presence of lung-sliding rules out PTX in the space observed, however the absence of lung-sliding does NOT rule-in PTX